19YR OLD PRIMI (36wks gestational age) with proteinuria
Case History and Clinical Findings






27/1/23RPR: NON RACTIVE HIV: NON REACTIVE 28/1/23: BT: 2MIN 30 SEC CT: 4MIN 30SEC APTT 38 SEC PT 19 SEC INR: 1.4 LDH: 200
19 YEAR OLD PRIMIGRAVIDA WITH 9 MONTHS OF AMENORRHEA CAME FOR SAFE CONFINEMENT. C/O SWELLNG OF BOTH LOWER LIMBS SINCE 10 DAYS LMP 19/5/22 EDD 26/02/23 POG 36 W 1D SEDD 25/2/23
HOPI:
PATIENT WAS APPARENTLY ASYMPTOMATIC 10 DAYS BACK, THEN SHE GRADUALLY DEVELOPED SWELLING OF BOTH LOWER LIMBS PROGRESSING TILL KNEES. RELEIVED ON TAKING REST AND INCREASED ON PROLONGED SITTING. NO H/O FACIAL PUFFINESS, DECREASED URINE OUTPUT NO H/O PAIN ABDOMEN, BLEEDING OR LEAKING PV, BURNING MICTURATION H/O FROTHY URINE SINCE 5 DAYS NO H/O FOUL SMELL INCREASED FREQUEMCY, URGENCY, POST VOIDAL PAIN NO H/O GENERALISED WEAKNESS, DYSPNEA, EASY FATIGUIBILITY H/O FACIAL PUFFINESS AND PEDAL EDEMA 3 MONTHS BACK, FOR WHICH SHE WAS ADMITTED AT KIMS AND TREATED.
H/O SIMILAR COMPLAINTS 1 YEAR BACK, FOR WHICH SHE WAS ADMITTED IN KIMS AND DIAGNOSED WITH NEPHROTIC SYNDROME AND USED T.WYSOLONE 60MG, INJ LASIX 40 MG, T. RAMIPRIL 2.5 MG AND SYMPTOMS SUBSIDED FOR 1 YEAR(USED FOR 6 MONTHS) H/O ANURIA AT AGE OF 7 YEARS WHEN SHE WAS ADMITTED AND TREATED IN A HOSPITAL H/O ?TB AT 6 YEARS OF AGE FOR WHICH SHE USED MEDICATIONS FOR 6 MONTHS
MENSTRUL HISTORY: AOM: 12 YEARS 5/30, REGULAR, NO PAIN, NO CLOTS.
MARITAL HISTORY: ML: 9 MONTHS, NCM
OBSTETRIC HISTORY: T1 CONCEIVED SPONTANEOUSLY, UPT DONE AFTER 20 DAYS OF MISSED PERIOD. FOLIC ACID TABLETS TAKEN, EARLY SCAN DONE. NO H/O FEVER WITH RASH, RADIATION EXPOSURE, BURNING MICTURATION, SPOTTING OR BLEEDING PV. DATING SCAN DONE. NT SCAN DONE- NFS. H/O DRUG USAGE FOR CONSTIPATION T2: QUICKENING FELT AT 4TH MONTH. TIFFA DONE AT 20 WEEKS 5 DAYS- NORMAL. 2 DOSES OF TT TAKEN. IRON AND CALCIUM SUPPLEMENTS TAKEN. NO H/O HEADACHES, BLURRING OF VISION, EPIGASTRIC PAIN. T3: PERCEIVED FETAL MOVEMENT WELL. NO H/O BLEEDING OR LEAKING PV, PAIN OR TIGHTNESS OF ABDOMEN.
PAST HISTORY:
K/C/O: HYPOTHYROIDISM SINCE 2 MONTHS. T. THYRONORM 25MCG, T. THYRONORM 50MCG ON MONDAY, TEUSDAY. N/K/C/O: HTN, DM, ASTMA, CAD H/O OROFER INFUSION 800MG 2 MONTHS AGO
FAMILY HISTORY
H/O RENAL DISEASE IN GRAND PARENTS?
EXAMINATION:
VITALS:
TEMP:97.5F,
HR: 96BPM,
RR: 17 CPM,
BP: 130/70 MMHG,
SPO2: 99%, GRBS: 77 MG%
HEIGHT: 146 CM, WEIGHT: 58 KGS,
BMI: 27.6 KG/M2
NO PALLOR, ICTERUS, CYANOSIS, CLUBBING, LYMPHADENOPATHY, PETICHIAE, PURPURA, CHEILITIS, GLOSSITIS, KOILONYCHIA.
JVP NORMAL
B/L PEDAL EDEMA PRESENT, PITTING TYPE, GRADE 2 P/A:
ABDOMINAL WALL EDEMA PRESENT UTERUS: 34-36 WEEKS CEPHALIC, RELAXED, LOA LIQUOR ADEQUATE CLINICALLY FHR +, 140BPM
GENERAL MEDICINE REFERRAL WAS TAKEN ON 28/1/2023 I/V/O S.TSH 87 ADV-TAB THYRONORM 75 MCG ON MONDAY AND TUESDAY TAB THYRONORM 50MCG ON OTHER DAYS ADV
ENDOCRINOLOGY OPINION. NEPHROLOGY REFERRAL WAS DONE ON 30/1/2023: ADV-EGG WHITES 2-3 PER DAY REVIEW WITH 24 HR URINE PROTIEN CREATININE RATIO AFTER 1 MONTH REVIEW SOS I/V/O INCREASED PEDAL EDEMA ,SOB
Investigation
27/1/23RPR: NON RACTIVE HIV: NON REACTIVE 28/1/23: BT: 2MIN 30 SEC CT: 4MIN 30SEC APTT 38 SEC PT 19 SEC INR: 1.4 LDH: 200
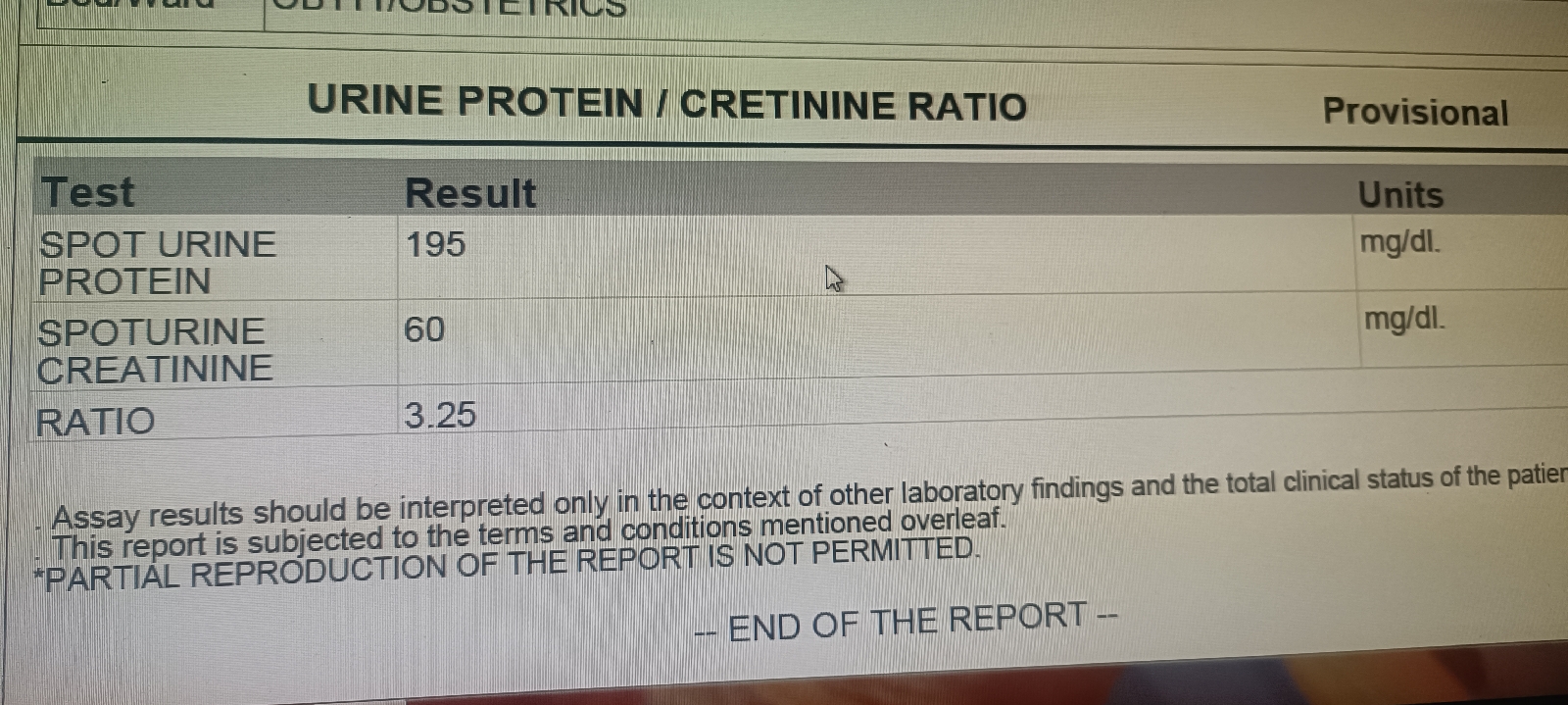
SPOT URINE PROTEIN CREATININE RATIO: 3.25 24 HR URINE VOL-1900ML
24 HOUR PROTEIN 2850
URINE C/S-NO GROWTH
OBS SCAN: SINGLE INTRA UTERINE ALIVE FOETUS IN LONGITUDANL LIE AND CEPHALIC PRESENTATION WITH ESTIMATED FETAL WEIGHT 2361+/-345GMS. FHR: 162 BPM
AFI: 11-12CM GA:33 WEEKS 5 DAYS ANC DOPPLER STUDY: NORMAL DOPPLER INDICES
Treatment Given
T. FERROUS ASCORBATE 100MG PO OD X 4 DAYS T. CALCIUM 1000MG PO ODX 4 DAYS T. MVT PO ODX 4 DAYS T. THYRONORM 75MCG PO OD X 2 DAYS T. SUSTEN 200MG PO ODX 4 DAYS GRD PROTEIN POWDER 2TBSP IN A GLASS OF WATER MILK PO ODX 4 DAYS
Advice at Discharge
PROTEIN RICH DIET SALT RESTRICTED DIET T. FERROUS ASCORBATE 100MG PO OD X 15 DAYS T. CALCIUM 1000MG PO ODX 15 DAYS T. MVT PO ODX 15 DAYS T. THYRONORM 75MCG PO OD ON MONDAY AND TUESDAY TAB THYRONORM 50MCG PO OD ON WEDNESDAY,THURSDAY,FRIDAY AND SATURDAY T. SUSTEN 200MG PO ODX 1 WEEK GRD PROTEIN POWDER 2TBSP IN A GLASS OF WATER MILK PO ODX 15 DAYS